A/T/N: An unbiased descriptive classification scheme for Alzheimer disease biomarkers.
Jack CR, Bennett DA, Blennow K, Carrillo MC, Feldman HH, Frisoni GB, Hampel H, Jagust WJ, Johnson KA, Knopman DS, Petersen RC, Scheltens P, Sperling RA, and Dubois B. (2016) A/T/N: An unbiased descriptive classification scheme for Alzheimer disease biomarkers. American Academy of Neurology, 87
One of the biggest hurdles for diagnosing Alzheimer disease (AD) and being able to distinguish between different types of dementia, is the fact that the diagnosis cannot be confirmed until a postmortem autopsy determines the changes in morphology of the brain and the location of neurodegeneration. Biomarkers, measurable indicators of biological state, are a more recent development and are crucial descriptive and diagnostic tools in diseases that do not have obvious physical manifestations, such as AD. They are able to demonstrate disease presence or the disease progression overtime in a living person. More importantly, the ability to study biomarkers has provided measurements of disease that previously could only have been evaluated post-mortem. Another obstacle present in AD research is that a consensus has not been reached as to a singular cause of the disease. The older AD pathology theories focus on β-amyloid and hyperphosphorylated tau tangle accumulation damaging the brain leading to a progression of neurodegeneration, however, the progression of AD has not been found to consistently be tied to an increase of β-amyloid or tau tangles. Because of this, Jack et al proposed a descriptive system that classifies 7 biomarkers of AD as either a biomarker of β-amyloid, tau, or neurodegeneration and neuronal injury working on a positive/negative system where a person is designated as having or lacking each. Here we will discuss the biomarkers of neurodegeneration.
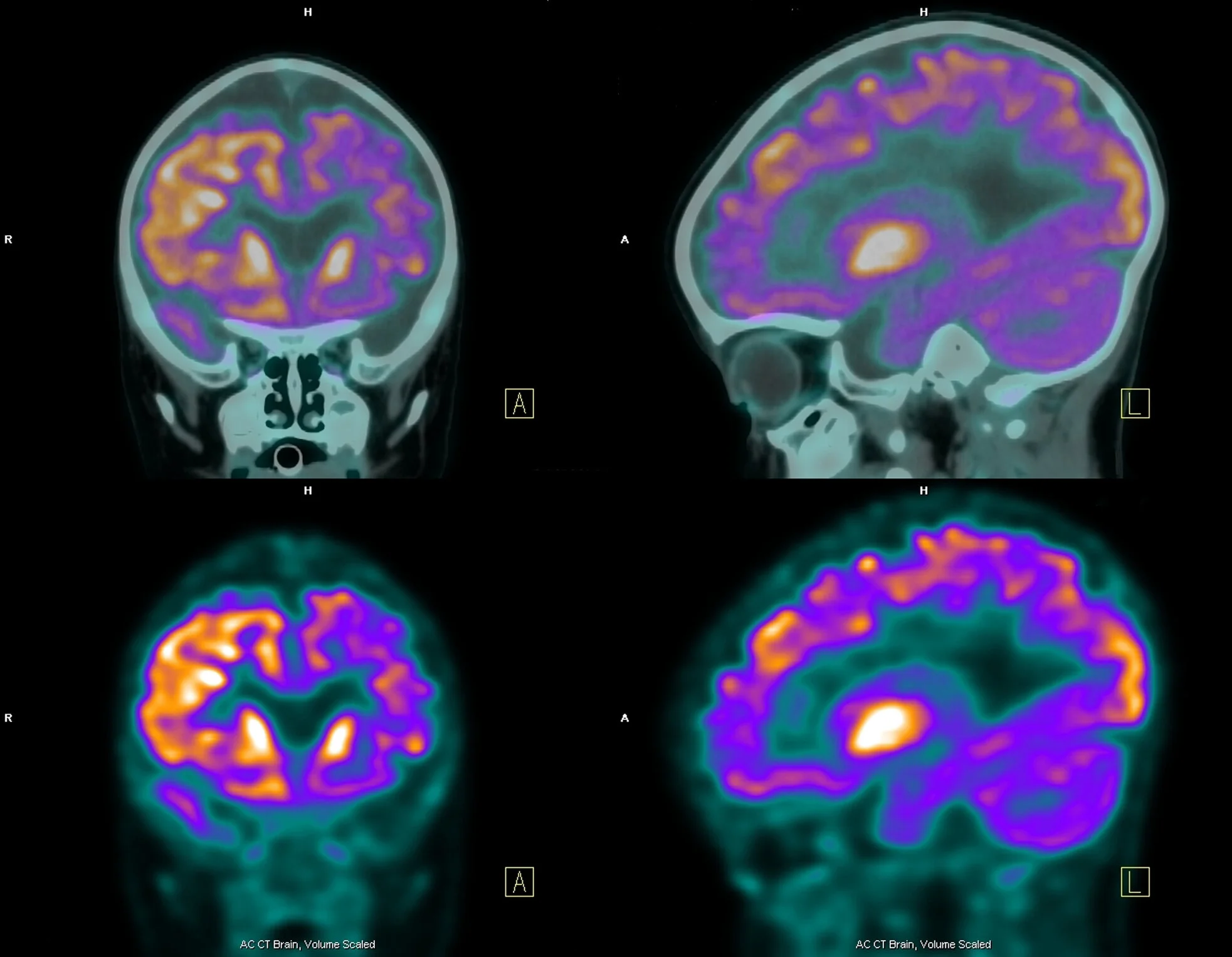
The biomarkers that Jack et al designate as demonstrating pathophysiology of neurodegeneration and neuronal injury are cerebrospinal fluid (CSF) total tau (t-tau), [18F]-fluorodeoxyglucose (FDG)-PET hypometabolism, and atrophy on structural MRI in the regions characteristically affected in AD. Having both CSF biomarkers and imaging as part of the classification gives both an absolute value to demonstrate abnormality but also an image to show the extent of the affects throughout the brain. AD often shows an increase in t-tau, but more significantly CSF t-tau is shown to increase in traumatic brain injury and stroke and correlates with the severity of damage. This indicates that CSF t-tau levels can reflect the severity of neuronal degeneration at a specific point in a person’s AD progression. [18F]-(FDG)-PET hypometabolism is used to measure the rate of glucose metabolism. The brain metabolizes glucose to function, therefore we can demonstrate brain damage if areas of the brain are not metabolizing glucose. Finally, atrophy is very characteristic of AD with cortical thinning, enlarged ventricles, and loss of hippocampal volume often seen due to neurodegeneration and loss of synaptic connections and neuronal branching. Although, both atrophy and hypometabolism are not specific to AD, they are found to behave similarly to CSF t-tau when compared to clinical symptoms. These biomarkers also allow clinical trials to study more treatment related outcomes. Historically, cognitive tests were the sole outcome compared longitudinally while the patient was alive, but these are often not objective. The ability to quantitatively demonstrate disease progression, stagnation, or improvement over time has been revolutionary in demonstrating treatment efficacy, or lack thereof.
β-amyloid and tau have been the main focus of AD research for decades, however there is a lot of conflicting data as to the true relationship between either and the pathology of AD as both are not always present when there is a clinical AD diagnosis. This would suggest that neither can be ruled as the driver of the phenotype. Jack et al provide reasonable critiques of the previously developed systems which often focus on β-amyloid and tau, stating that separating the biomarker findings from an associated temporal order (ie. β-amyloid occurs first and encourages the spread of tau, and presence of tau is associated with neurodegeneration, thus the three must occur in this order) and clinical impairment may be more applicable across all AD clinical diagnostic states, even those mildly impaired or lacking proteinopathy. In addition, they point out that with increasing age comes an increased potential for AD, non-AD, and mixed brain pathology. A more descriptive classification, such as the A/T/N system, will provide a wider acceptance and include more of the aging population than previous classification systems, most of which require the presence of β-amyloid. As the three categories are independent from each other, further categories could be added, such as the presence of more proteinopathies which could allow this system to be used for other neurodegenerative diseases such as Parkinsons’s disease. Other categories that Jack et al suggest could be added in the future are synaptic dysfunction and cerebrovascular disease. Although it will take time to fine-tune the independent categories included, the A/T/N system will provide a straightforward system that could distinguish different manifestation patterns between the different dementia and AD types.